
After performing over 500 Brazilian butt lifts and helping guide global BBL safety standards, I can tell you that fat grafting is one of the most technique-dependent procedures in plastic surgery. Results vary widely from surgeon to surgeon, and most surgeons never see each other’s work, so comparison is nearly impossible. But you can compare results, and you should.
The questions that follow are the ones I would want a family member to ask. They expose how a surgeon actually operates, and they will help you pick the best BBL surgeon. They cover four areas: credentials and safety, surgical technique, expected results, and outcomes. These are the questions you should be asking if you are considering a Brazilian butt lift.
If you ask nothing else, make sure you come away from your BBL consultation with answers to these three things:
- Does the surgeon hold board certification specifically from the American Board of Plastic Surgery?
- Does the surgeon inject fat exclusively above the muscle fascia?
- Is the BBL surgery performed in an accredited facility?
A surgeon who cannot answer all three directly is not meeting the current standard of care. Here is the full list of questions to consider for your BBL surgery:
1) Are you board certified by the American Board of Plastic Surgery?
This is the first question you should ask any plastic surgeon, for any procedure. Ask it precisely. Not “are you board certified?” but “Are you board certified by the American Board of Plastic Surgery?“
There are many surgeons who are board certified in other specialties, or who are certified in cosmetic surgery by boards that are not accredited by the American Board of Medical Specialties. They take advantage of patients’ lack of information to appear as though they are board certified by the American Board of Plastic Surgery, but they are not. Read more about the difference.
If they are not being transparent about this, should you trust them with your surgery?
For BBL specifically, this matters beyond credentials. Plastic and reconstructive surgery residency is where fat grafting technique is taught and refined under supervision. Surgeons from other specialties have not completed that pipeline. They do not receive the safety guidelines from the Plastic Surgery Board. For a procedure where technique directly determines both your result and your safety, that distinction is not paperwork. It is patient protection.
You can verify any surgeon’s ABPS certification yourself at abplasticsurgery.org before your consultation.
2) Where is the surgery performed, and what accreditation does the facility hold?
The facility matters as much as the surgeon. A 2022 analysis of BBL-related deaths in South Florida, published in the Aesthetic Surgery Journal, found that 92% of fatalities occurred at high-volume, budget clinics. Not in properly accredited surgical centers.
Ask directly: What accreditation does the surgical facility hold? Look for QuadA, AAAHC, or a state-licensed ambulatory surgical center designation. Then verify it yourself before your consultation.
At our practice, all surgery is performed at Cosmetic Surgery Facility, LLC, a QuadA-accredited, Medicare-certified private surgical center that I founded, built, and operate as Medical Director. It is not a shared facility or a hospital. Learn more about our surgical center.
3) What type of anesthesia do you use, and who administers it?
This question does not get asked often enough, especially for a procedure that runs 5 to 8 hours.
Ask what type of anesthesia will be used, and who will be administering it. At our practice, the standard for Brazilian butt lift is IV sedation, sometimes called twilight anesthesia, similar to what is used for a colonoscopy. You are deeply relaxed and will not remember the procedure, but you breathe independently throughout. No ventilator. No intubation.
The reason this matters clinically goes beyond comfort. General anesthesia causes vasodilation, which means the veins enlarge. The ventilator also uses positive pressure to push air into your lungs, which forces blood out into the peripheral veins, dilating them further. Larger veins mean a bigger target for injury during fat injection, and an easier pathway for fat particles to enter the bloodstream. That is a risk factor for pulmonary fat embolism. With IV sedation combined with tumescent solution, the opposite happens. The veins actually get smaller, making vein injury harder and fat entry less likely.
I do not think Brazilian butt lifts should be performed under general anesthesia. I have held that position for many years and have spoken on it at ASPS national meetings. Read more about BBL risks and the case for IV sedation.
As for who administers the anesthesia, board-certified anesthesiologists and CRNAs (certified registered nurse anesthetists) are not equivalent. Ask specifically which one will be in the room with you. At our surgical center, all anesthesia is administered by board-certified anesthesiologists only.
4) How do you perform the Brazilian butt lift?
You want to have the surgeon explain their technique so that you understand how they perform each phase. The Brazilian butt lift has three distinct parts: liposuction, fat processing, and fat reinjection. Each component is critical to the success of the entire surgery.
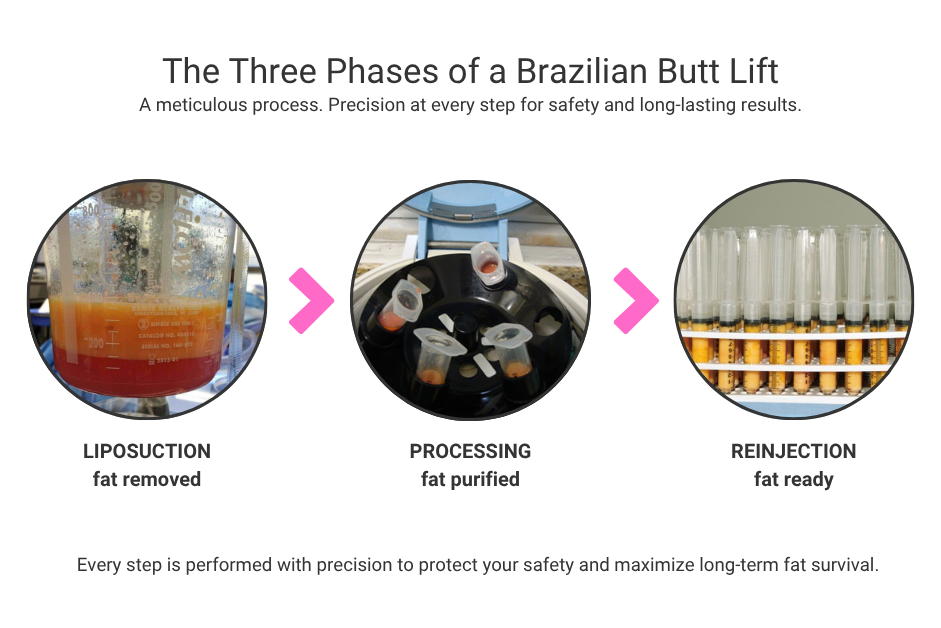
Liposuction
Fat removal should be done with a fine, thin cannula at low suction pressure to preserve the delicate fat cells and get smooth, even liposuction results. Typically, a total of three areas of liposuction are performed. If a large cannula is used, the fat will come out faster, but the liposuction results may not be smooth. The use of a thin cannula will make the procedure longer, but the results should be better.
Fat Processing
The fat should be centrifuged at low gravity forces for brief periods of time. If not, debris and unhealthy or dead cells will be mixed in with the good cells used for reinjection, and the fat will not last.
Fat Reinjection
Fat should be reinjected in small quantities using fine cannulas, the micro-droplet technique. Fat injected in large deposits does not integrate properly with surrounding tissue and will not hold long term. This approach takes longer. That time is not wasted.
I have been advocating for the micro-droplet technique and against power injection methods since 2017. The 2022 joint safety advisory from multiple plastic surgery societies has since validated that position. Power injection methods, where fat is delivered in large volumes per pass using a mechanical pump, prioritize speed over precision and make it difficult to control exactly where the fat is deposited. Large bolus injections increase pressure and the risk of fat entering the vascular system. The micro-droplet technique is not just about fat survival. It is a safety issue.
5) Where exactly do you inject the fat, and do you use ultrasound guidance?
This is the most important technical question you can ask, and it is directly tied to your safety.
Fat must be placed exclusively in the subcutaneous layer, the tissue just beneath the skin, above the gluteal muscle fascia. It must never be injected into or through the muscle.
Here is why this matters: large gluteal veins run through the muscle like this:
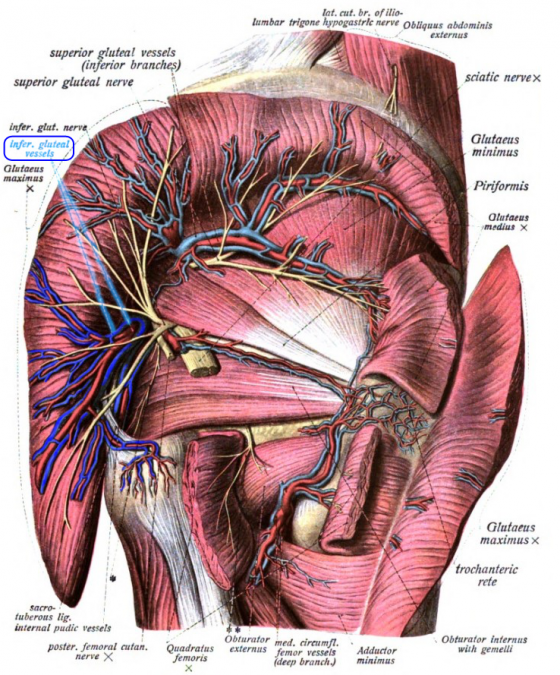
When a cannula penetrates the muscle and fat is injected under pressure, fat can enter those veins and travel to the lungs, causing a pulmonary fat embolism, a complication that is nearly universally fatal. As one of 19 plastic surgeons selected worldwide to serve on the Multisociety Gluteal Fat Grafting Task Force, I reviewed the autopsy findings firsthand.
Every deceased BBL patient had the same findings: fat in the gluteal muscles, damage to the gluteal veins, and massive fat emboli in the heart and lungs. No confirmed death involved fat that remained exclusively in the subcutaneous plane. The 2018 task force advisory identified intramuscular injection as the cause of every confirmed BBL death at that time, with a mortality rate of approximately 1 in 3,000.
Once the mechanism was understood, the surgical community acted. By 2019, the vast majority of plastic surgeons had transitioned to subcutaneous-only injection and the mortality rate dropped dramatically. The August 2022 joint safety statement from ASPS, The Aesthetic Society, PSF, and ASERF formalized subcutaneous-only injection with real-time ultrasound guidance as the standard of care.
Ask your surgeon: “Do you inject fat exclusively above the muscle fascia?” The answer you are looking for is yes, subcutaneous only, above the muscle. It should come without hesitation.
Then ask: “Do you use real-time ultrasound guidance during fat injection?” Ultrasound removes the uncertainty that tactile feel alone cannot eliminate, even for experienced surgeons. If the answer is no, ask why. Experience alone is not a sufficient answer. Any surgeon you consult with should be able to answer both questions without hesitation.
6) How long will my BBL surgery take?
Because of the meticulous way the fat has to be extracted, processed, and reinjected to get a permanent result, the surgery is time consuming. Typically, a Brazilian butt lift will take 5 to 7 hours. If a surgeon quotes you less than 4 hours, they are taking significant shortcuts. For context, the 2022 South Florida analysis found that surgical times at high-volume budget clinics averaged approximately 90 minutes. That is not a Brazilian butt lift. That is a shortcut with consequences.
Here is how the time breaks down:
- Liposuction of 3 areas: minimum 2 to 3 hours
- Fat processing: varies and can be done simultaneously
- Fat reinjection: minimum 2 to 3 hours
You want to have a feel for time in surgery because shortcuts compromise quality and result in less predictable outcomes. Typical shortcuts that compromise results are harvesting fat with large cannulas instead of thin ones, not centrifuging the fat to separate debris and dead cells, and injecting the fat too fast or in large quantities. Any of those shortcuts can result in poor surgical outcome, or results that do not last.
While you are asking about time, ask how many Brazilian butt lifts the surgeon performs in a day. At 5 to 7 hours per case, the math is straightforward. A surgeon performing four or more in a single day is not giving each patient the time this procedure requires. The 2022 joint safety statement explicitly raised concerns about high case volume per surgeon per day for exactly this reason.
Finally, make sure you know who is performing every part of your surgery. If another surgeon or assistant is involved in the liposuction or fat injection, that person must also be board certified in plastic surgery. A surgical tech should not be doing the liposuction or the fat injections.
7) What BBL complications have you personally seen, and how do you handle them?
You are not looking for “none.” You are looking for honesty, specifics, and a clear protocol.
Every surgeon who has performed a significant volume of BBLs has seen complications: seromas, asymmetry, contour irregularities, fat necrosis. A surgeon who says otherwise either has not done enough cases or is not being straight with you. What matters is whether they have a clear, practiced response when something goes wrong, and whether their facility is equipped to handle it.
8) How many Brazilian butt lifts have you performed?
Press for an actual number, not a range. A surgeon with real volume can tell you.
Then ask to see before and after photos of at least 10 good results, and look for variety. There should be slender cases, mid-range body types, and heavier patients in the mix. This shows the surgeon has experience with difficult cases, and gives you a better chance of finding a body type you can identify with.

9) What is your idea of the best BBL result for me?
The best BBL result addresses the whole body, not just the buttocks.
You should expect the surgeon to address how your whole body looks, not just enlarge the butt. The waist to hip ratio is very important, so I also pay attention to the hips and discuss with every patient whether fat should also be injected into this area.
Too many patients focus on volume of fat retention or how many cc’s they want rather than what looks good. The objective is to have a great looking body, not just a big butt. Ask the surgeon to describe what they think will produce the best result for you specifically, paying attention to your whole body, not just your booty.

10) How much of the transferred fat survives, and is it permanent?
Patients like to ask this question, and I understand why. It would be helpful if I could give you a reliable number to look for. The honest answer is that no surgeon can, and not because they are being evasive. The tools to accurately measure fat survival simply do not exist.
Complex MRI studies have shown survival rates ranging from 30 to 70 percent, but even that range reflects how difficult fat survival is to measure. Any surgeon quoting you a specific number is offering an educated guess. A surgeon promising something close to 100 percent is a red flag.
What the research does agree on is that survival is almost entirely technique-dependent. How the fat is harvested, processed, and injected determines how much takes, which is exactly why the questions above matter. Post-operative care plays a role as well. Protecting the grafts from pressure during the early healing period is critical.
Here is what I can tell you from my own extensive experience: fat cells that successfully establish a blood supply in the surrounding tissue are permanent. They become part of your body and behave like native fat for the rest of your life. Since 2005, I have not had to reinject a single patient because transferred fat was absorbed.
Fat that takes correctly does not reabsorb over time. Which is exactly why the next question about revision rate is the most reliable indicator of how confident a surgeon actually is in their technique.
11) What is the likelihood I will need a revision or touch-up?
This is the acid test.
If a surgeon tells you a touch-up is possible, plan on it. If they are vague about redos, they have probably done more of them than they want to discuss.
Touch-ups and redos become necessary because the fat is reabsorbed, which is caused most frequently by taking shortcuts in technique. After over 500 Brazilian butt lift cases, including more than 200 large-volume cases (over 400cc per buttock), I have not had a single patient who has needed a redo because of a graft loss. The only patients who returned for more surgery were satisfied patients who had gained weight since their original surgery and wanted more fat injected for an even bigger result.
Ask for the practice’s explicit policy on billing for touch-ups and revisions before you commit. A second round BBL should have a significant discount. However, your initial Brazilian butt lift is no bargain if you need a redo.
12) How much does a Brazilian butt lift cost, and what does the price include?
Ask for a clear breakdown before you commit to anything, and make sure you understand exactly what is and is not included. Surgeon fee, anesthesia, facility, post-operative garments, and follow-up visits should all be accounted for. Some practices quote a base price and add fees later.
At our practice, pricing is transparent and all-inclusive. See current BBL pricing and what is included. Financing is available, including 6-month no-interest options. See our financing page for details.
📋 Taking these questions into your consultation? Print the checklist.
Dr. Ricardo L. Rodriguez is a Yale-trained, board-certified plastic surgeon, certified by the American Board of Plastic Surgery with over 30 years in practice. He is one of 19 surgeons worldwide appointed to the Inter-Society Gluteal Fat Grafting Safety Task Force and a 2026 Castle Connolly Top Doctor, recognized in the top 7% of physicians nationwide by peer nomination.
A Brazilian butt lift is more than just adding volume. It is about sculpting proportion and balance. With over 500 procedures performed, Dr. Rodriguez treats patients from across the United States at his Baltimore practice, focusing on safe, natural-looking results using meticulous fat transfer technique. His approach to gluteal fat grafting, centered on subcutaneous-only injection, was published as a chapter in Plastic and Aesthetic Regenerative Surgery and Fat Grafting (Springer Nature, 2022).
Dr. Rodriguez is fluent in English, Spanish, and French. Contact us to schedule an in-office or virtual consultation. Virtual consultations are available for out-of-town patients and for second opinions. Call 410-494-8100.

Schedule a Consultation with
Dr. Rodriguez
Originally published June 3, 2013.



{kind=link}
Madeline Frets says:
Dr. Ricardo L Rodriguez says:
Madeline Frets says:
Dr. Ricardo L Rodriguez says:
Ana pappas says:
Dr. Ricardo L Rodriguez says:
Ivy D. Pabon says:
Dr. Ricardo L Rodriguez says:
Olivia says:
Dr. Ricardo L Rodriguez says:
Olivia says:
Dr. Ricardo L Rodriguez says:
Robyn says:
Dr. Ricardo L Rodriguez says:
Heather Shimp says:
Dr. Ricardo L Rodriguez says:
Heather Shimp says:
Dr. Ricardo L Rodriguez says:
Tammara Littleton says:
Dr. Ricardo L Rodriguez says:
Rosa says:
Dr. Ricardo L Rodriguez says:
Sara says:
Dr. Ricardo L Rodriguez says:
Yolanda says:
Dr. Ricardo L Rodriguez says:
Alejandra says:
Dr. Ricardo L Rodriguez says:
Tricia says:
Dr. Ricardo L Rodriguez says:
Jessenia says:
Dr. Ricardo L Rodriguez says:
Hope says:
Dr. Ricardo L Rodriguez says:
Anonymous says:
Dr. Ricardo L Rodriguez says:
Lashawn says:
Dr. Ricardo L Rodriguez says:
lora maldonado says:
Dr. Ricardo L Rodriguez says:
Lisa says:
Lisa says:
Dr. Ricardo L Rodriguez says:
Danisha says:
Dr. Ricardo L Rodriguez says:
Rhiann says:
Dr. Ricardo L Rodriguez says:
Keisha says:
Dr. Ricardo L Rodriguez says:
Melanie says:
Dr. Ricardo L Rodriguez says:
Melanie says:
Melanie says:
Dr. Ricardo L Rodriguez says:
Asia says:
Dr. Ricardo L Rodriguez says:
mya says:
Dr. Ricardo L Rodriguez says:
Mary says:
Dr. Ricardo L Rodriguez says:
Sue says:
Dr. Ricardo L Rodriguez says:
Maly says:
Dr. Ricardo L Rodriguez says:
Olga says:
Dr. Ricardo L Rodriguez says:
kendra bailey says:
Dr. Ricardo L Rodriguez says:
Michelle C says:
Rose A says:
Dennece Leist says:
Dr. Ricardo L Rodriguez says:
Patriciah Mutombgwerah Tigere says:
Dr. Ricardo L Rodriguez says: