Patients routinely get fat grafts to the face, breast, and buttocks. However, some patients do not get the results they wanted because the fat graft did not ‘take.’ So, what happened? Why do fat grafts sometimes die (or fail to ‘take’)? In this post, I will explain one of the most important factors in creating a long-lasting fat graft.
When the recipient tissue is normal, there really should be no need for a touch-up, or revision. Plastic surgeons have all of the tools they need to create a good fat graft on the first try!
What is fat grafting?
Fat grafting, aka Fat transfer, is a process which removes fat from one area (the donor area) and transfers it into another area where enhancement is desired (the recipient area). The procedure involves these three steps:
- Removal of fat from the donor site using liposuction techniques
- Decanting/centrifugation of the extracted fat
- Re-injection of the processed fat into the area receiving enhancement
All three steps are important to fat graft longevity, and a deficiency in any one of the three steps can result in poor fat graft retention. I have previously discussed the best protocols for decanting and centrifugation (step 2), so today I would like to specifically address the best methods for removing fat from the donor area (step 1) in order to yield a fat graft that has high retention, with a long lasting result. In other words, this article focuses on the best Liposuction technique to extract the fat, which is then used to create the fat graft.
Fat extraction from donor site
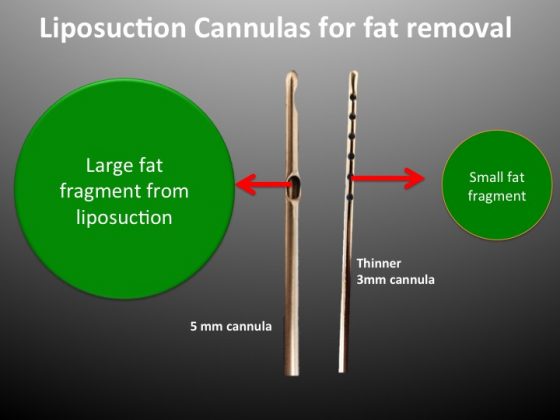
In the fat removal process, a surgeon’s primary tool is the liposuction cannula. These are the long slender rods that the surgeon uses to extract the fat from the stomach, love handles, back, and other anatomical regions with fat deposits. The cannulas come in different sizes and they have different size holes near the tips. The holes are the areas through which the fat enters the cannula from inside your body.
Cannula size
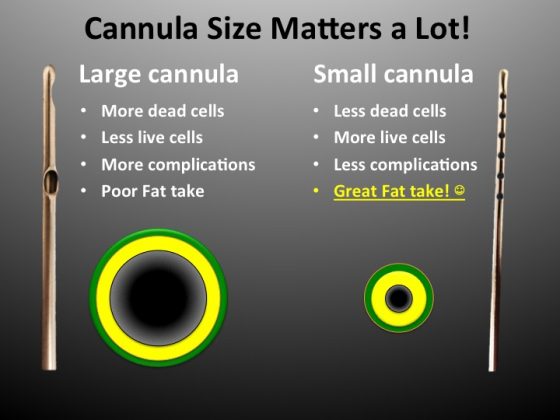
In the plastic surgery community there is a lot of talk these days about whether you should use large (5mm) or slender (3mm) cannulas for liposuction. If you have read my blog posts in the past, you know I have a preference for using the thin, 3mm cannulas. There are other surgeons, however, that insist larger cannulas are better.
SMALLER fat particles make BETTER fat grafts!
With respect to their use in fat grafting: Is the size of the cannula a matter of opinion or is it something that can be verified by science?
A recent publication by a prominent plastic surgery researcher concludes that smaller fat particles make better fat grafts. This has huge implications for the type of cannula that should be used for liposuction as part of the fat grafting procedure!
Size of fat particles influences fat graft retention
In an article published by the Plastic and Reconstructive surgery journal with Dr. Kotaro Yoshimura as the lead author, the answer is unequivocally that small fragments of fat are better for fat graft survival (or fat graft ‘take’).
Dr. Yoshimura determined that small fat particles have a higher concentration of viable fat cells than large fat particles. Compared to small fat particles, large fat particles have a higher volume of necrotic or dead cells.
The takeaway message from the article is that you want the liposuction cannula to remove the highest concentration of small fat particles to get the best fat graft take.
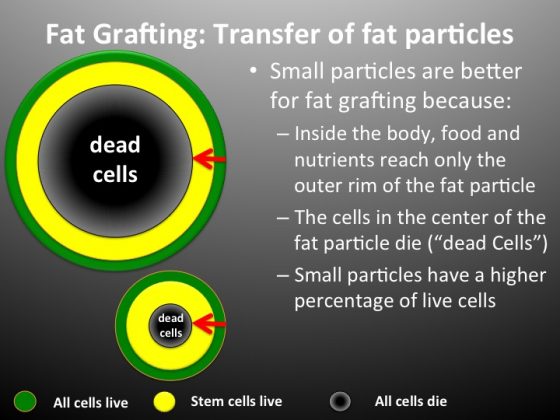
To visualize the areas described in Dr. Yoshimura’s paper, think of a fat particle as a small sphere, or small ball of fat. In the diagram above, the three regions of a fat particle are shown with different colors. The outermost portion of the fat particle is green, the innermost portion is black, and the region between the inner and outer shell is yellow.
Because of their position near the surface of the particle, the cells in the outermost green zone of the fat particle gets lots of nourishment inside the body. In other words, the cells that are on the outside rim of a fat particle are the cells that are the most viable and will survive in a fat graft. Dr. Yoshimura found that cells in the yellow area will yield a mix of viable, repaired, and dead fat cells. The black zone is the innermost area of any fat particle, and it is referred to as the necrotic zone. Inside the body these fat cells do not get any nourishment and are dead from the start. The fat cells in this zone make poor contributions to fat grafts and should be avoided.
A closer examination of Dr. Yoshimura’s article details that the necrotic, or black zone, starts at a depth approximately .6mm from the outside perimeter of the fat particle. This would apply to any size of fat particle. Since the good viable fat cell zones are somewhat narrow and close to the edge, large fat particles would therefore have huge black zones of necrotic cells.
How to get small fat particles during Liposuction
A liposuction cannula is a long, hollow rod with holes located at the end. A lot of attention has been placed on the diameter of the rod (3mm vs 5mm), but I feel that for fat grafting longevity the size of the hole in the cannula is even more important than the diameter of the cannula.
Compared to a 5mm cannula, a 3mm cannula will give smoother, finer extraction results for the donor area (stomach, etc). However, it is the cannula hole size which will dictate the viability quality of fat cells which are used for the fat graft. The cannula hole is the first contact point with the fat particle inside the body. A small hole will only accept small particles.
Therefore, I feel the best combination for extracting fat is a 3mm diameter cannula with 1mm holes at the tip. If you have a piece of fat that is about 1 millimeter in diameter, a large percentage of the fat cells will survive, there will be very little inflammation, and most of the fat graft will take. That is why I use a cannula that has the smallest hole possible, which is a 1mm hole. That way I am sure I harvest small, 1 millimeter diameter, pieces of fat.
If a surgeon uses a larger 5mm cannula with larger holes to extract the fat, the fat graft may be doomed from the start. With big holes, the fat graft particles will be larger than 1 millimeter in diameter and a large proportion of the cells in the graft will die.
Take the example of the thick, 5mm cannula with 3mm hole openings.
Remember, only the cells in the outer .6 millimeter rim stand a chance of survival. Large particles will have huge necrotic zones and make poor contributions to the fat graft. Likewise, these necrotic cells can cause inflammation, loss of fat graft, and in some cases scarring, cysts, or other complications.
This is not a matter of surgeon preference or opinion. This is science. Ask your surgeon what type of cannula he uses to harvest fat for your fat graft. If he is using larger cannulas to remove the fat, he is not giving you your best shot for a successful fat graft.




{kind=link}